“The outcome of any serious research can only be to make two questions grow where only one grew before ” ~ Thorstein Veblen
As a new study on surrogate mothers was published last month we were inspired to look at various research that has been done over the years and was struck by one from 1994 that I read some time ago when I came to this topic. The 2022 study – with surrogate mothers in America, engaging with surrogacy under a commercial model – appeared to be both similar and different, to the women from a study nearly 30 years ago in the UK who were having a baby for someone else, for ‘altruistic reasons’.
Here we compare and contrast both studies and as these are just our observations we encourage readers to read the original studies and the other studies listed.
Published in Dignity last month, findings from a survey and in-depth interviews of 96 surrogate mothers between 24-50yrs were analysed.
These are my top 3 key findings in this study:
- The women were 3 times more likely to have a caesarean section
- They were 5 times more likely to go into early labour
- Surrogate mothers are “more likely to experience postpartum depression following the delivery of surrogate children than after delivering their non-surrogate children.”
With maternal mortality in the US remaining an issue for women, particularly for women of colour, it’s clear that surrogacy pregnancies are more likely to have both physical and mental health challenges, compared to pregnancies that are not for others.
“We found that surrogate pregnancies are more often labelled as high-risk pregnancies independent of maternal age or gravidity. This research supports the findings of Woo et al. (2017) in that surrogate pregnancies had a higher rate of delivery via Csection. Women were more likely to deliver at an earlier gestational age compared to their genetically related or spontaneous pregnancies.”
Of 141 pregnancies recorded in this survey, 157 babies were born, so ‘multiples’ of twins (or more) were present in this cohort and the highest number of complications, (such as pre-eclampsia, gestational diabetes, haemorrhage, infection related to pregnancy, pre-term labour, hyperemesis gravidarum, anaemia, placenta previa, placental abruption etc) in one pregnancy was 7.
To support their findings researchers reference existing studies:
“In their study, Duffy et al. (2005) documented significant obstetrical complications of ten gestational surrogate mothers. Almost a decade later, Merritt et al. (2014) sought to determine the impact of assisted reproductive technologies (ART) on pregnancy-related outcomes, including surrogate pregnancies. Their research found a fourfold increase in stillbirths, a fourfold increase in cesarean sections for mothers who used ART and a nearly fourfold increase in preterm birth (Merritt et al., 2014). Another study by Woo et al. (2017) looked at pregnancy outcomes of gestational surrogate pregnancies alone. It examined the records of 124 surrogates and found a significant difference in physical outcomes between their own spontaneous pregnancies and their gestational surrogate pregnancies.”
As well as pregnancy, birth and post-birth issues, such as post natal depression (which is 37.5% more likely in surrogacy pregnancies vs 4% in non-surrogacy pregnancies), I was interested in the educational background and financial circumstances of the surrogate mothers in the study.
It showed that Surrogate Mothers by and large, educated but economically disadvantaged and therefore likely motivated by the payments they will receive for the baby they grow and give birth to.
“Of the 96 women, 69 were employed at the time of the interview and the median annual family income reported was $85,000 (minimum income of $13,000 and maximum income $225,000—quite a large range). In addition, 74 of the 97 women had some post-secondary school education: 17 had an associate degree, 42 had a bachelor’s degree, 14 had a master’s degree, and 22 were high school graduates. Only one woman did not complete high school. No women had completed doctoral degrees. Of the 87 women who had a husband or a partner, 50% of the partners had a high school education or associate degree.”
The commercial aspect of surrogacy in the US results in obvious ethical concerns , but this otherwise apparent problem is often rejected as an issue for UK surrogacy due to the so-called ‘altruistic’ model we have in law. However, education, employment and level of income are intrinsically linked. Additionally, as noted in our Egg Donor Blog, the payment for ‘expenses’ can be central to the decision making. This is the same with surrogacy ‘expenses’. Women who have contacted us tell us that the regular monthly payments for ‘expenses’ are key factor in their decision to have a surrogacy pregnancy. The US study remarks:
“Interestingly, women were less likely to admit that money was the motivating factor for entering into a surrogate arrangement, but held the belief that other women who enter into these arrangements are motivated by the money it offered. Regardless of perceived motivation, women in this study were more likely to use the payment they received to get out of debt or pay bills and none of the participants were in the upper tiers of taxable income.”
In the UK study from 1994, only 19 surrogate mothers were interview. Aged between 20-30 yrs the surrogate-born children they gave birth to made up roughly half the population of this cohort of babies at the time (all singleton births but for one set of twins and ongoing pregnancies). As the UK law had only been introduced less than a decade prior, and with the popularity of surrogacy at the time in no way reflecting the levels of surrogacy we have today in the UK, this can only serve as a snapshot in time.
Titled “I wanted to be interesting. I wanted to be able to say I’ve done something interesting with my life“ the study aims to look at awareness of surrogacy as well as the reasons for engaging in surrogacy and the relationships that resulted for these women. There was some scepticism of IVF as at the time wasn’t as widely used as it is today. Artificial Reproductive Therapy (or ART) was considered a new technology. Interestingly, one surrogate mother refused to transfer parental rights as she didn’t perceive the parents as suitable by the end of the pregnancy, another conceived through sexual intercourse (or what is now known in some donor conception circles as ‘natural insemination’, or unprotected full sex).
Whilst the majority of the women in the American study were educated and employed, in the UK study the vast majority of women had no higher education and in fact may have not completed school.
“Fourteen of the women had left school at age 16 or earlier and only one had remained in full- time education to age 18, although nine had undertaken further vocational and educational studies, often on a part-time basis-combining study with employment and/or motherhood. Five women had left school with no format educational qualifications, the remainder gaining qualifications to GCE; and CSE level at least. For two women advancement through educational qualifications was an expressed priority and for whom the need to finance further education was a major motivating factor in becoming a surrogate mother.”
Despite the status of surrogacy allegedly being for ‘altruistic reasons’ two women sought it out for the purpose of investing in their education as to advance, or ‘escape,’ their current circumstances.
“I needed some money and it seemed an easy way to gain a large sum. Secondly, I loved being pregnant but didn’t want to look after any more children … Once I am qualified and able to make money in a more acceptable way there is no possibility of me considering surrogacy again even though [it has] been most exciting and rewarding. I looked at it as a way of getting out of the poverty trap.”
Understandably, money, regardless of location, education or business model, remains a primary factor drawing women to surrogacy. This study noted that two women saw surrogacy as a “reasonably convenient” way of ‘earning’ money whilst being a stay-at-home mother and as recently as 2015, Kim Cotton from COTS was ‘recruiting’ women for surrogacy as a practical method to earn money as a stay at home mother. (For background, Kim Cotton is a UK resident who agreed to have a baby for an unknown couple from America before there was Uk law on surrogacy. She was paid £6,500 at the time.)
However over half of the UK women thought that money was not (and should not be) – the prime motivating factor. One commented that there were easier ways of making money, such as refusing to relinquish the child and selling their story! Laws regulating surrogacy were not a decade old when these women were interviewed but it mentions “ evidence of both sensitivity and ambiguity concerning payment.” This has been clarified by the 1998 Brazier report as “reasonable expenses”.
The study says:
“It is unrealistic to expect surrogate mothers to carry a pregnancy and hand over a baby (or babies) to the commissioning parents without reimbursement of expenses at least, in recognition of their time (e.g. loss of earnings), the inconvenience, discomfort and risks to which they were exposed, and additional costs incurred.”
So even under a ‘altruistic’ model, a ‘service’ payment was incorporated into the considerations of the sum. Expenses should ‘at least’ be paid, alongside a loss of earnings and exposure to risk. Now we see payments being referred to as ‘expenses’ but it’s unclear how an ‘expense of pregnancy’ is defined. From the Law Commission consultation it was noted that in 2015 only 4.4% of surrogate mothers were claiming in the £15,000 – £20,000 bracket, but by 2018 this increased nearly 10% to 14.6%.
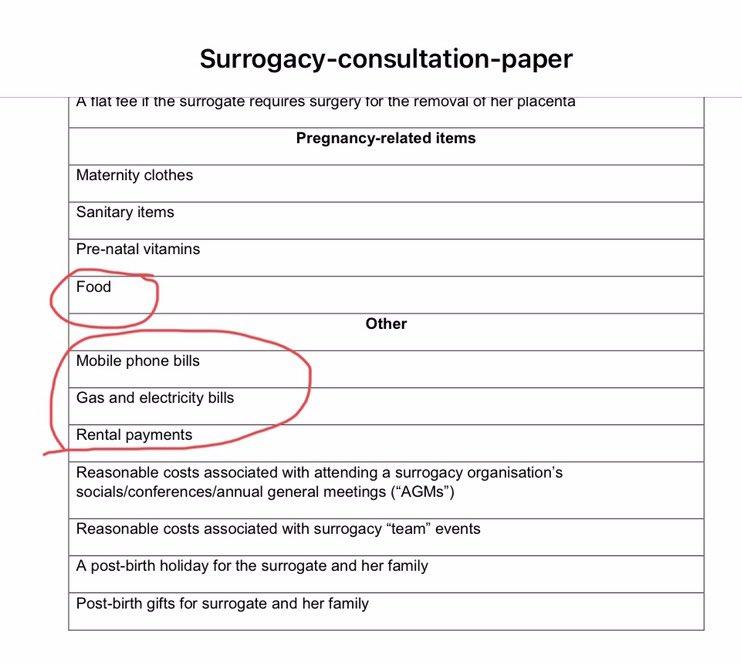
Have the lines become blurred to disguise a payment as an ‘expenses’ to to make surrogacy more socially acceptable under an altruistic model?
(Regarding loss of earnings, it’s important to note that Maternity and Parental Leave didn’t come into effect until 1999 in the Employment Act so this study pre-dates this and in 2022, America’s maternity provision falls far short of the UK’s.)
The difference in the US study was that over half of the women had degrees but were stay at home mothers and it is unsurprising that military wives are a cohort of surrogacy candidates. A perfect example is La’Reina Hyanes, the surrogate mother for one of the Kardashian/West children. According to Heavy.com La’Reina has a degree in criminal justice but was a stay at home mother of two young sons at the time, her husband worked in the military and one of her sons has a medical condition. The US health system would require money for her son’s treatment and would be a strong motivating factor for a surrogacy pregnancy. Her second surrogacy pregnancy was for the Kardashian/West couple who paid her $45,000 over 10 months.
As was explored with our blog on BBC 3’s The Surrogates, we agree with the US study as…
“A great deal more could be done to study the financial incentive on the decision to become a surrogate mother”. The UK study highlights altruism as 11 women specifically identified the “pleasure and joy” given to the commissioning parents as the “best part” but there was an underlying sense of being kind or worth present.
“I wanted to do something that was out of the ordinary and that made me a little bit special. And I think, because I haven’t got a lot of confidence, I’m not a mathematician or anything like that, I’m not a world-class model, and just normal. And I didn’t want to be normal, I wanted to be interesting. I wanted to be able to say “I’ve done something interesting with my life.”
This sentiment is mirrored in some of the stories we hear from the women who have contacted us and for me it is worthy of exploring as in a wider context, I have a sense that there is possibly some form of ‘toxic femininity’ contributing to a women who see their value in their fertility and their ability to produce children.
There appear to be some trends in both the situations and circumstance of the women who engage in surrogacy as well as the motivating factors involved in their choices. We aim to return to explore this further but no-one says it better than Janice Raymond. She argues that altruism, though mistaken for agency, “has been one of the most effective blocks to women’s self-awareness and demand for self-determination”. Altruism for women must be put into context to be fully understood.
Another reason given was what we might recognise today as obstetric violence and a need to rectify mistreatment from a previous pregnancy.
“It’s given me the chance to experience a pregnancy and a birth where I’m in control, not the doctors…. I know what I’m doing this time and I’m not going to allow things to be done to me that were done to me in my previous pregnancy.”
Both studies make reference to respect and relationships and the US study highlights some interesting statistics on respect in maternity care and extended family:
“Participants, on average, reported feeling respected 88.1% by intended parent(s), 85.5% by the agency, and 90.3% by healthcare staff.”
“My first two surrogacies, I felt very respected (100%) by the intended parents and the agency, but my last surrogacy I [felt] very disrespected (0%).”
“When you are pregnant with your own, everyone wants to help you, but, with my surrogacies, my in- laws didn’t want to help me at all—and my co-workers were annoyed because I got time off after my surrogate delivery because ‘It’s not your baby.’”
“My care team giving birth was amazing, but I was discharged less than 24 hours after birth. Nobody asked me if I was okay or how I was feeling.”
The UK study looked in detail at the relationship between parties and future contact.
“Whatever had been decided jointly at the outset with commissioning parents agreements concerning future contact, telling the child the truth about her or his conception and birth, and the payment of expenses, may not be kept. However, they recognized that they could do little about this other than trust the commissioning parents to keep their word.”
Referring to the children born of surrogacy and genealogical bewilderment, some of the women wanted to stay in the life of the child they gave birth to.
“I was adamant that I would never bring a child into the world and it was going to be lied to. I’ve had friends who were adopted and told at 16 and I’ve seen them crushed. It must be awful. And I said “I’m not prepared to be party to any of this. It’s to be told as soon as it starts asking questions at 2 and 3. It’s to be made as normal as possible, no big deal”. And we all agreed on that. And that was probably the first thing which caused the underlying problems … I discovered when I was pregnant that [the commissioning mother] was pretending to be pregnant to her family.”
In the conclusion it is stated that all the surrogate mothers felt some continuing responsibility for the future well-being of the children they had helped to bring into the world. Five surrogate mothers feared their involvement in the child’s life would only serve as a “constant reminder” and cause confusion or distress. There were two cases at the time of the interviews where contact was about to cease due to strain and the stress of the relationship.
“It should not be assumed that parting with the child was unproblematic. Five mothers spoke about their sorrow and distress about parting with the child, and for two this was described as the worst part whilst one husband described his worst part as recurrent fears that his wife – having conceived – would change her mind about relinquishing the child.”
So where one woman may be occupied with thoughts of how to give the baby to the commissioning parents, her partner or husband is concerned that she may be unable to do so. Personally, I recognise the impact on other members of the family, including the surrogate mother’s other children.
Two surrogate mothers experienced surrogacy regret.
“If somebody came up to me and said that they wanted to be a surrogate mother I would do my damnedest to talk them out of it. I don’t think I’d ever recommend it to anyone again.”
Similar sentiment was expressed in the US study.
“I suggest to every woman who thinks about becoming a surrogate: please consider another way, whether it’s for the money, or the delusional idea of self-fulfilment, or whatever. You’re not just hurting yourself, you’re hurting the baby you carry inside you as well.”
To conclude (thank you for reading this far!), research is important. It informs policies and laws. 28 years apart, both studies explain their limitations and call for further research. We can obtain, statistics and facts, work out percentages and averages and at the same time recognise that each person has their own experience and this cannot be summed up as a number. But we also can recognise that each woman has their own individual experience that cannot be summed up as a number or a percentage. Nor does quantitative data always give us the fullest picture in light of more women’s narratives.
The women we hear from make up a miniscule percentage of the UK population but their experiences of surrogacy regret is of no lesser value than those who it works out for. For every happy ending there could be an equal number of stories of loss and regret, we simply don’t know. How do these numbers stack up, how many would you comfortable with, if laws are further relaxed…maybe 10 women with regret, maybe 100?
As the UK Law Commission prepares to deliver it’s report this Autumn we look forward to reading their recommendations that will draw from the public consultations and other research, as this will inform the reform of UK law that is likely to follow. We also eagerly await the outcomes of a study currently underway into the voices of the children born from surrogacy.
In both studies I reviewed there were women who did it for money, but not necessarily only for the money. A desire to help, to be useful, to give something to someone to realise their dreams of parenthood – all can be true whilst also being paid for your ‘service’. The line of where that payment is for expenses compared to what earns you a different future can be thin. This must also be weighed against how much is too much for ‘reproductive service’ and does this mean that the final product, a newborn baby, equate to a trade in children and yet another method of exploitation in women?
Is surrogacy baby buying or a kindness only women can offer? What happens when the arrangements made isn’t what you thought it would be and you want to change your mind? What happens when the child isn’t ‘perfect’ and the commissioning parents change their minds? Is it reasonable for surrogacy to be funded on the NHS, similar to IVF treatment? Should parental rights be transferred at birth and how much control could then be exerted over the pregnant woman?
It is lawmakers who get to decide on the policymaking around surrogacy. These are men and women who have been elected and constituents are invited to write to their MPs to express their concerns around these practices.
For more on these issues, please subscribe and follow us on Twitter. @WombsNotForRent.
