In the digital age, social media platforms have become a sprawling landscape for connection and community but for every well-meaning and helpful group there is a flip-side. Online groups occupy the dark corners of the internet where bad actors take advantage of the vulnerable. As the annual 16 days for the Elimination of Violence Against Women and Girls (EVAG) draws to a close, we turn our attention to social media surrogacy groups as this year UN Women calls for an “End to digital violence against all women and girls”.
The alarming escalation of violence against women found online extends to surrogacy as this harmful practice is a form of violence against women, as clarified by the UN Special Rapporteur for VAWG in her report this year. Here, I examine the risk posed by online groups, primarily on Facebook.
These groups are dangerous for several reasons. They perpetuate the illusion of empowerment through bodily autonomy with subtle language which encourages women to help others and create ‘positive change’ in the world. Women are told they can (and should) share their fertility, spread the joy of family and ‘give a gift’ of a baby to someone, somewhere who cannot, for whatever reason, have a baby themselves.
For many women considering surrogacy, the prospect of helping others whilst providing a solution to financial difficulty is a no-brainer. The promise of financial ‘compensation’, coupled with the chance to help a family achieve their dream of parenthood, presents surrogacy as a noble act of altruism, the ultimate kindness. But these groups are predatory and deceptive as they hide the deeper exploitative practices. Clinics and agencies entice women in and then make direct approaches, often switching to Direct Messages to dictate the terms and conditions. One woman who got caught up in these groups told us that she wanted to offer herself to a couple abroad as she trusted legal systems in other countries, more than those in her own.
This single mother was offered money for a positive pregnancy test, more than double that for the heartbeat, more money again for accommodation, transport, a ‘feeding allowance’ and lastly, vastly increased sums for a twin or triplet pregnancy. At no point were the known risks discussed.
“I really wanted to do it all for my child to have a better life…after helping a family I’d come back to run my business” recognising her narrow escape in a country fraught with exploitation she told us, “I may have been used for a human trafficking scam”.
Advertising for surrogacy in the UK is illegal but these online groups present a loophole. Where would this illegal action be prosecuted, the UK where the post was viewed or in the country where the platform is registered? How and where should these groups be reported? I have personally reported several predatory groups to Facebook and no action has been taken. A journalist in Nigeria has had better luck. Simbiat Bakare’s investigation resulted in closures of several surrogacy Facebook groups (and we encourage readers to report any concerning posts, particularly those that offer a payment plan, by reporting under the category of ‘sexual and human exploitation’ and then selecting ‘exploitation of people under 18’).
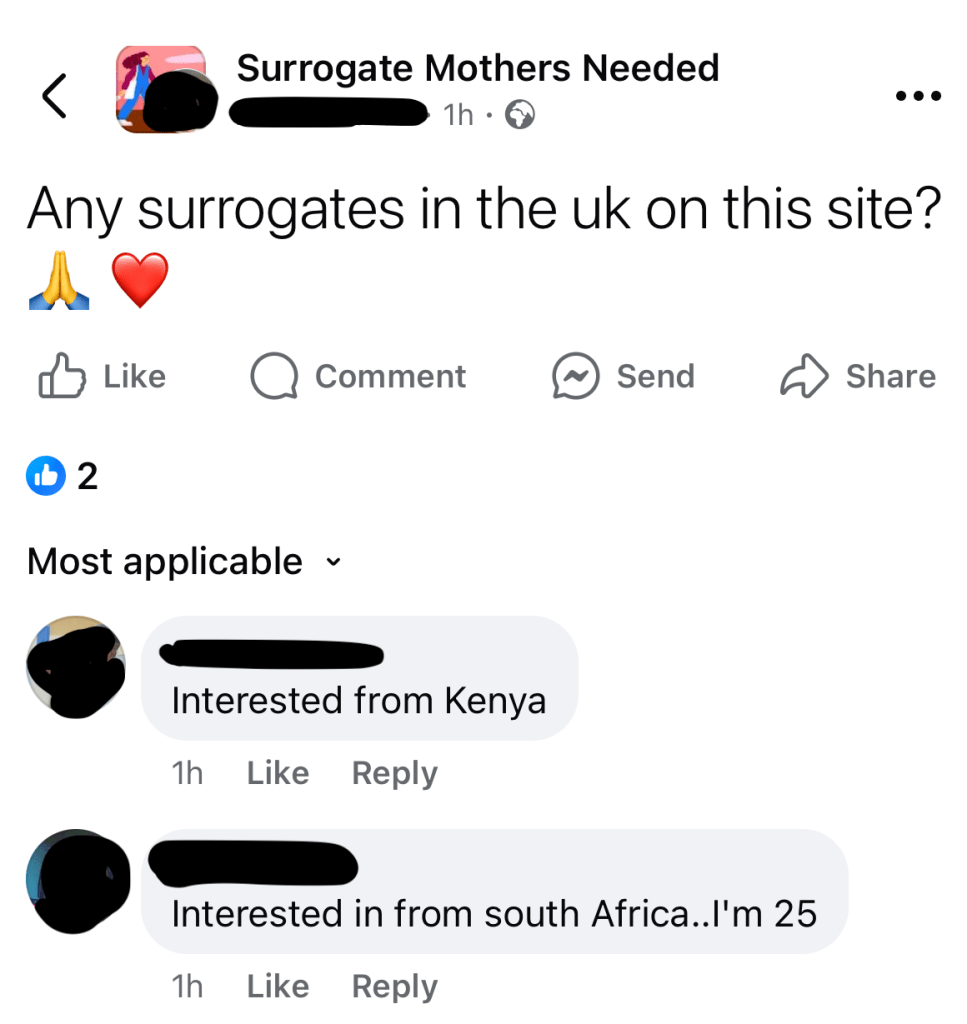
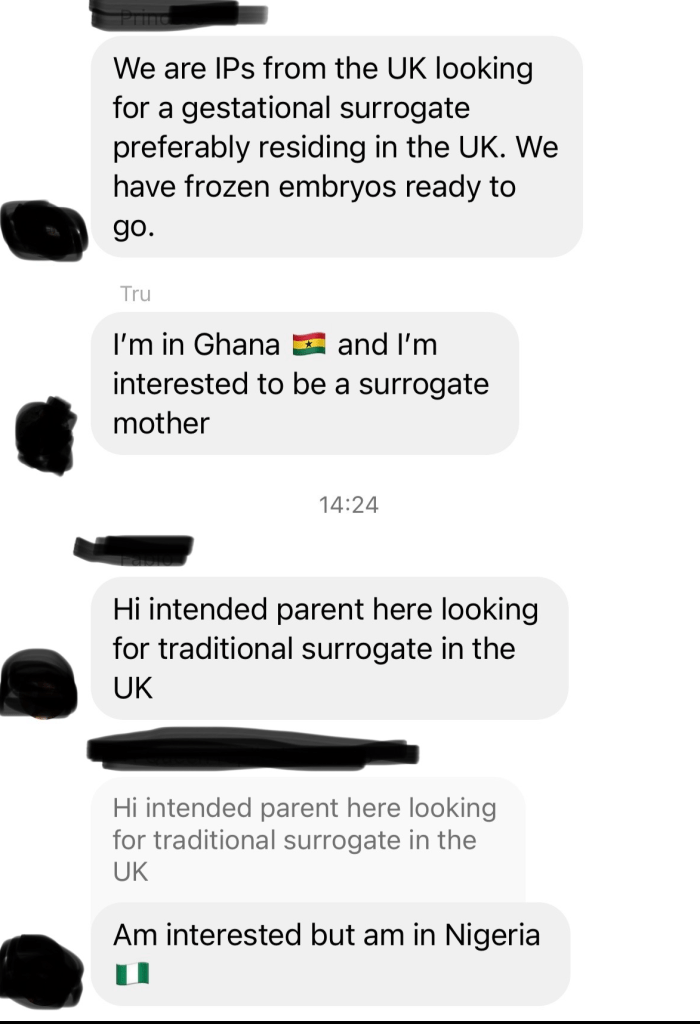
Both couples and single people can post about their desire to be parents and invite potential candidates to message them directly. Professional ‘matchmakers’ have private groups and we often see vulnerable women who are already navigating financial challenges, leap at the chance of being able to earn money this way. By making an arrangement with strangers online a woman can go through a pregnancy, birth and give up parental rights for her newborn in order to support the children she already has.
We understand why this is attractive and have seen countless replies to adverts, mostly from women in Ghana, Nigeria and South Africa, who intend to travel abroad to earn large sums that are simply not available to them at home. The possession of a passport and willingness to travel is mentioned in their replies.
In surrogacy, women are reduced to mere vessels that meet the desires of wealthier individuals or couples, this power imbalance is plain to see from the thousands of screenshots I have seen personally and it exposes a troubling reality. Here are just a handful of examples.
The allure of money overshadows the real emotional and physical risks involved in carrying a child for someone else. Playing on their vulnerabilities, agencies and brokers will dress this up as making someone’s dreams come true. How wonderful it must be, to be making wishes a reality for a hopeful couple who badly need your help. You have something they don’t and they are willing to pay for something that comes relatively easily to you. And by doing this lovely, selfless act, you can support your family and even work your way out of poverty.
It’s a harmless win-win for all! But the agencies brokering deals never mention the risks.
I was reminded recently of how it took decades for warnings to be attached to cigarette packets and tobacco companies were marking their own homework as they provided the ‘research‘. (The predictable outcome of these ‘studies’ resulted in more sales and profit for Big Tobacco as the risks were hidden so smokers thought they were safe to carry on.)
Facebook groups also foster personal narratives that create a false sense of sisterhood (more on this soon) that also downplay the real dangers. The idealised version of surrogacy minimises the significant risks and the transactional nature of these arrangements reinforces this power dynamic and rather than challenging them, these online communities allow surrogacy to fester and grow, unchecked.
We must remain vigilant against those that seek to commodify women’s bodies for profit and challenge the predatory nature of these exploitative groups. Instead of arguing for surrogacy as a reproductive right, that it is an act of generosity made possible with bodily autonomy, we should say no to it all, so vulnerable women do not take risks with her own lives, their own fertility and their own wellbeing for true empowerment without the biased influence.
Handmaid’s Tale, Chanel 4 – Season 6 (The irony of this image is not lost on me.)
My name is Marie-Anne Isabelle and the surrogacy experience that I endured here in this country nearly killed me. My mission now is to ensure that nobody goes through what I did. I have made it my cause to expose this barbaric practice for what it is and to enact change. I am not looking for glory or sympathy I just want change.
People hear about how wonderful surrogacy is, how it’s a beautiful gift and a positive experience. Then, you hear about the “terrible” surrogate who dares to ask for her child back. It’s an all-too-common depiction in our modern fairy tale world.
I believed that fairy tale when I agreed to help a family member by carrying her child. At the time, I was happy to help because I loved her and did not want or need to be paid. However, I made it clear that the child would be conceived using her egg and that I must be allowed to see and have contact with the child I would give birth to. That was the condition I would only do this under, if I could have regular contact with the child, as I could not live without seeing a child I would give birth to.
I agreed to become a surrogate mother for my cousin. She was more like a sister to me. She had been a significant presence in my life. We were a vital part of each other’s lives. I knew about her cancer. In 2009 she told me that she had created embryos and that she was researching surrogacy.
One day, she came to my house with her sister, who is also my cousin and asked if I could help her. I told her that I would only help if she let me see the child. She looked me in the eye and said, “Absolutely. There’s trust.” We’re family, you know? Not for a minute did I think I’d actually need to get a lawyer and write a contract.
I think when she asked me, she knew I had no choice but to say yes. I think she exploited our relationship. As further information came out afterwards, it appeared that they couldn’t go ahead with a surrogacy abroad as it was deemed too expensive, so they were looking for a cheaper alternative. They kind of saw me as “Oh, she’ll do it for free.” A free and cheap option.
I was told there is trust. “You will be the child’s godmother.” Those words would later come back to haunt me. I don’t believe she knows what trust means. She made all sorts of promises to brainwash and coerce me into helping her.
It was a gestational surrogacy. They used IVF with their own biological material. I remember lots of injections and visits to the clinic for very obtrusive physical examinations. It was a very procedural process, and it was quite challenging, both emotionally and physically, to go through. I’d had two normal, non-assisted pregnancies of my own and this pregnancy was nothing like those. This overmedication was purely to help these two people.
The experience was bad enough. Having somebody else try to dictate what medical procedures you should endure, how you should give birth, and what you should eat was awful. The list goes on. This affected me from the beginning of my pregnancy, yet there is still no specialized support for women going through surrogate pregnancies here in the UK.
In 2014, at the time of delivery, I made it clear that the commissioning father wouldn’t be present; it would just be her, me, and my partner. Everything went smoothly, and I felt in control. The hospital saw me as the mother. So, my wishes were taken into account; in how I wanted to do things. However, they wanted me to have an elective C-section. I refused, and my midwife backed me up by stating that C sections were not good practice. If someone doesn’t need one, they shouldn’t have one. They tried to force me and put pressure on me, saying, “Oh, it’d be better for you.”
I remember there being some confusion at the hospital. Even though the hospital had been told that it was a surrogacy, social services became involved. I thought, “This is awful. I’m trying to have a baby, and now I’ve got suspicious social services interviewing me.
The father came in after the birth because he wanted to have skin to skin contact. They had the baby. They were happy. They didn’t need me anymore so they told me to go home. However, the hospital staff did not agree. They wanted to see me walk out with the baby, carrying it according to their policy. I remember having to carry the car seat with the baby in it through the hospital in full view of the medical staff. Then, we had to do this strange exchange where I handed over the child in the hospital car park because, legally, the hospital was no longer responsible for the child once it was outside.
After the birth, I was presented with all sorts of legal documents that I was forced to sign. The timing was awful, too, right when I was trying to recover from the birth. Imagine training your body and mind for nine months to believe that you are not the mother of the child you are giving birth to. Every surrogate woman has to do that. Then, after doing that, you are presented with a document stating that you are the mother, and you are forced to sign it. I was also threatened with financial and legal consequences if I didn’t sign it. This is the dark side of surrogacy in the UK that nobody hears about because most women are given gag orders to prevent them from talking about it.
No payment was made. I was only compensated for time off work. I remember them buying me maternity clothes and reimbursing me for transportation to the clinic. They wanted to pay for food, but I politely declined. I didn’t want to feel controlled by having someone tell me what to eat. I remember my dear cousin saying, “We’d like to pay for a kitchen for you,” and I said, “No, this is me helping you I am not doing this to get anything back in return. For me to receive gifts would feel like I was being paid for a service.” I said no.
The court case started in 2014 and lasted two years. I didn’t start the court case. It was initiated by the commissioning parents because they wanted a parental order. A parental order legally transfers parental responsibility from the surrogate to the intended parents and ends the surrogate’s rights.
I had no idea about any of this. I didn’t even know there was going to be a court case. I just thought I would hand the child over and be done with it. None of this was made clear to me beforehand. Nobody told me. I gave birth, and suddenly, all of this legal process was forced upon me. I refused to sign because they reneged on their promise of allowing me contact and everything went downhill from there.
They attempted to obtain my consent against my will at the court, exploiting my mental health, which was irreparably damaged as a result of my experience. They tried to prove that I was incapable of giving consent. However, through grit and determination—including psychiatric assessments proving I was capable of giving consent—I was permitted to remain involved in the court case and my consent was needed much to their dismay. Still, they continually tried to shut me out. Children’s Services even tried to use the case of a deceased surrogate mother. They said, “We can just use that case where someone died and pretend that’s happened here.” It was just appalling. It was made clear to me that the only way I had the best chance of having any contact was to agree to the parental order so in the end, I signed it to try and have contact with the child I gave birth to as I was promised. I have never seen the child to this day.
She was born in 2014. I haven’t seen her since I gave birth to her.
I was promised on multiple occasions during the court case that I would see her, but each time, the appointment was cancelled the day before. They were playing games with me. I believe the promises were only for the benefit of the court.
They hinted that they used me as a cheap commercial surrogate and if it hadn’t been for their legal costs they would have been granted their wish. They constantly tried to remove any trace of me from their child’s life, which is another reason why they needed my silence. I believe their behaviour stems from their resentment of me as the child’s birth mother, and that is me being generous.
I have been diagnosed with complex PTSD and underwent EMDR to alleviate some of the trauma resulting from the surrogacy. I have a deep fear of hospitals, children, and babies, which does not work well with my career in education. The damage done to me will never be repaired. Constant panic attacks and a fear and distrust of people serve as constant reminders. There are many days that I still wish I wasn’t here just to be rid of this painful world that did this to me.
The impact was not only on me, but also on my children. They took on the role of parents because I wasn’t able to take care of them. This happened ten years ago, and for the first five years, my children didn’t have a mother. They were taken away from me and sent to live with their father, which was traumatic for everyone. Then, the judge, when presented with evidence, came to the conclusion that this was not helpful to anyone and returned them to my care. Over the last five years, we have come together as a family and rebuilt our relationships, but for the first five years, we were a broken family.
In trying to help another family, they broke mine.
When did a women’s right to have a child mean that it would take away another woman’s right to have contact with a child she gave birth to? We talk about women’s rights as if they are universal but surrogacy actually means you are choosing which woman deserves more rights. That is inequality.
If leaders and law makers care so much about women’s rights why are they continuing to erode the rights of surrogate mothers?
Change needs to happen fast. Surrogacy in any form is wrong, not safe and harmful. It needs to be banned before any more women die as they already have. Listen to our voices and do not let us be silenced any more.
This speech was read by Marie Anne at FiLiA in Brighton on 11th October 2025.
Last month we received a ‘cease and desist’ letter from a law firm on behalf of their clients, My Surrogacy Journey.
This UK agency wanted us to stop talking about them and the law firm representing them issued a SLAPP – a Strategic Legislation Public Participation. Frowned on by the Solicitors Regulatory Authority, a SLAPP aims to intimidate and silence opponents. It sends a message to recipients that speaking further may land them in legal trouble.
Since I have not done anything illegal I will continue to write about this agency and their connected businesses such as their new clinic, their foundation, their agency in Mexico and the Modern Family Show which is paused as they await the birth of their third child, born to a woman in Mexico this time.
But I am not at all surprised that an agency operating under the UK model of so-called ‘altruistic’ surrogacy whilst running a commercial operation in Mexico, might not appreciate my words in this article, which inspired the letter. No, I am not surprised at all as we have seen the active silencing of women who speak up about surrogacy before.
Several surrogate mothers who were signed up with Surrogacy UK have told me they were removed from groups after raising doubts, concerns or for expressing feelings doutb, reluctance or regret. As this doesn’t align with their narrative they were ejected and blocked. These women can no longer access the social networks designed to support them, they have no one to talk to outside of their own friendships and family, and as surrogacy is presented as a unique and alternative way to have a family, many do not understand the intricate and complex emotions that come to a head in a surrogacy pregnancy and postpartum.
We supported a surrogate mother through part of her legal ordeal which was thankfully successful in ‘setting aside’ the parental order she signed under judicial encouragement. The judgment handed down prevents her from speaking publicly and she is not the first, nor will she be the last.
Another surrogate mother has been threatened more subtly, by calling her character and reputation into question and should she continue to speak out her credibility will be undermined. Others may want to speak but they don’t have the freedom to discuss their experiences and this is not a new experience. Surrogate mother’s in the USA fear being sued if they speak out. A 2015 UK court case saw a surrogate mother banned from speaking to the press after a judge’s decision saw her baby placed into the care of the genetic father, and his partner, against her wishes:
Similar gagging orders are issued in other countries that apply the so-called ‘altruistic’ surrogacy model. A 2017 case in Canada saw a rapid agreement following an online meeting and a contract that prevented her from speaking out:
“the couple offered her $500 to forego legal advice in order to speed things up….The document was also written to make the arrangement appear completely altruistic on the part of the surrogate, even though she would be paid a set amount of money whether or not she actually incurred expenses.”
Alison Motluk writes “But what bothered me most was that she was strictly forbidden from revealing any of it. The contract contained a gag order.”
Alison Motluk has written on the regularity of surrogate mothers being ‘gagged’ and shares lines from contracts detailing where surrogate mothers cannot share anything about their ‘journey’.
In some countries the threats go beyond a legal letter or a court ruling. Some surrogate mothers are threatened with the loss of their lives. An international contact of ours who wishes to remain anonymous told us:
“Mothers are afraid to speak because agencies are very powerful and there are countries where it is very easy to make a woman disappear, because their lives are worth nothing. Earlier this year a 25 year old woman acting as a surrogate mother bled to death in an illegal clinic. This happened in a country where surrogacy is legal. The mafia are threatening the family to keep silent, forcing them to delete social media posts and stay silent after the death of their loved one.”
We are often asked, why don’t these women say something, but is it any wonder as to why you don’t hear their stories when legal rulings, contracts, agencies and legal threats prevent them from sharing what happened to them?
We are one of only a handful of organisations in the UK representing the other side of surrogacy. We are not funded, we do not charge for membership and we do not receive donations. We do not have money to pay lawyers but we do have is an abundance of time to listen to surrogate mothers.
I invite all surrogate mothers with regret, doubts or concerns, to reach out to us by email (or DM us on Twitter/X) to share your stories with us in confidence. We understand why you have not been unable to speak and we are here to listen to you and what your experience of surrogacy has been.
And the cease and desist letter? Well, when someone wants you to stop talking about them as you’re making them look bad, that’s reason enough to carry on and perhaps shout even louder.
There has been considerable attention to a paper by a Norwegian philosopher, Dr Anna Smajdor, in the journal Theoretical Medicine and Bioethics, outlining the case for what she calls “whole body gestational donation” (WBGD) as a form of surrogacy. This astounding paper was picked up first by Reddux, and since has received attention not just on social media but also in publications such as the Daily Mail and Cosmopolitan. The reaction is, in the main, mostly one of astonished revulsion, with a few voices as shown here (see the comments under the Daily Mail article).
The gist of Dr Smajdor’s argument is as follows: In 2000, Rosalie Ber suggested that women who have been diagnosed according to the brain death criteria, or who are in a persistent vegetative state (PVS) could be used as gestational surrogates. Yet, “surprisingly”, says Smajdor, this seems not to have been implemented anywhere in the world. Smajdor makes a few adjustments to Ber’s proposal, limiting it to women diagnosed as brain dead, and argues that with prior consent of the woman, it could provide a useful means to achieve pregnancy for those unable to carry a child to term, or, indeed, as an alternative to pregnancy for any woman, given that pregnancy is not entirely risk free. The existing system of organ donation is used to justify this, hence the description of “whole body gestational donation” which sees this as analogous to donating separate organs or body parts to save life or improve health in other individuals. Much could be said in comment on this paper but here we will simply make a few remarks…
Firstly, there are many reasons why this proposal does not seem to have been implemented, one of them being the high cost of sustaining a patient on life support, which would mean that to initiate and sustain a pregnancy until viability would be likely to involve costs in the hundreds of thousands of pounds if not more.
The high costs, plus other practical problems, does mean that this form of surrogacy may never be used in practice. But this does not imply that we should be complacent. One reason for concern is that such extreme proposals are often used rhetorically in debate. A troubling scenario is suggested. There is a general outcry. Then along comes the counter response: “We are not going to do anything so terrible! We agree this is going too far. We are proposing we do something far more reasonable!” Or perhaps, often later once the fuss has died down a bit, “We will do this, but don’t worry, we’ve listened to concerns, we’ll do it only with safeguards.”
But the proposed policy may be “far more reasonable”, may have “safeguards”, but is still nonetheless full of problems. “Not so bad”, may still be not good enough.
And a second reason for concern is that even if Smajdor’s proposal is never adopted, the ways in which she argues, including her view of childbirth, and of the human body in general and women’s bodies in particular, are firmly representative of much mainstream influential thinking in bioethics. There are many commonly used ways of arguing and of thinking about ethical problems which tend to skew towards certain “rational” sounding solutions, often favouring the use of new technologies, but which frequently present only a very limited and biased view of matters. Let’s look at just a few of the problems with Smajdor’s reasoning, problems which occur again and again in the field of bioethics.
We can start by looking at the analogy with organ donation, because it will alert us to some major problems. The argument goes by analogy:
X is really the same as Y. We accept Y. So we should accept X, in order to be consistent.
We accept organ donation. So we should accept donating the whole of one’s body, not just parts. Otherwise we are being irrational. “Those who accept brain stem death as an adequate basis for organ donation, should for consistency acknowledge its acceptability for WBGD as well”, opines Smajdor.
But Smajdor has actually shot herself in the foot by using organ donation as her model, because everything we know about organ donation confirms that human beings are not simply “rational” creatures, and the body is not merely a machine to be broken into spare parts.
Rates of organ donation are critically dependent upon sensitivity to the feelings not just of the donor but crucially of their families. Critical accounts in the media can greatly impact rates of donation, and sensitivity and empathy in explaining the situation and requesting consent of relatives is vital. Spain is often held up as having a particularly successful organ donation and transplantation system. This may be credited to its “soft opt out” system where the default position is that of consent, but critical to this is the extensive training in communication and sensitivity for those involved in requesting permission from families. Critical too, is widespread public understanding and acceptance, respect for those who opt out, and widespread agreement on the good that is being done by successful transplantation. (Remember the controversy that George Best had a liver transplant, only to continue drinking.)
How we treat the dead, including those who donate bodies, tissues or organs, is a deeply ingrained part of human culture. The very earliest signs of human civilisation show elaborate concern for proper burial. Disrespectful treatment of the dead has been used to mark disdain for enemies and criminals. But this, we now find abhorrent, showing how strong our respect for the dead is even in our “rational” and “scientific” age. We are moved to find that elephants also show respect for their dead. We cannot wave away these concerns with a few so-called “rational” arguments.
But this is precisely what Smajdor seems to do in her paper.
Smajdor acknowledges that in WBGD, the focus will move from caring for the patient, to using the patient’s body as a “repository of tissues that can be used to benefit others”. But, she says, this is just what happens anyway in organ donation.
Yes, it is. This is precisely why extreme sensitivity is needed. This is precisely why a different medical team deal with donation, not the team caring for the patient. This is precisely why, ideally, trained staff communicate with and care for the family. All this is overlooked in the name of “rational consistency”.
In the world of pure reason, truths are universal and eternal. Smajdor has no sense of time as for her it makes no difference. She recognises that in organ donation, we have to extend ventilation after brain death is diagnosed to keep the organs in a healthy state before they are removed for transplantation, and that in whole body gestational donation, this time would be extended. “But ventilating someone for two days, two weeks, or two years makes little difference except insofar as it forces us to acknowledge what we are doing before we hasten onto the next stage,” she writes.
But we are creatures who live in time, not in the abstract world of reason. Our experience of time is, well, an essential part of our lives, is woven into our entire embodied existence and development, our lives, our birth, our death.
Indeed, for families of those who donate organs, the time their relative spends on ventilation, and the harvesting of organs, does make a significant difference. The manner in which the family can say goodbye changes. This is not to be dismissed, and the generosity of families who willingly agree to this for the sake of others should be acknowledged. Smajdor seems to think that the issue can be resolved into overcoming our “distaste” for sustaining brain-dead patients for long periods. The “discomfort” here, she suggests, “relates to the liminal state between life and death that brain-dead patients occupy”, as if overcoming this discomfort is akin to, say, overcoming squeamishness at having to pull a splinter out of someone else’s fingernail.
For the rest of the human race, these “liminal states” are the stages of transition between life and death which form critical points of significance and meaning. The recognition of their significance is an integral part of our humanity. Neither at the start, nor at the end of life, does Smajdor understand the importance of how we respond to our embodied existence.
Furthermore, Smajdor has a pick and mix approach to evidence. She bends over backwards to examine the minutiae of the scarce empirical evidence regarding gestation in women who are diagnosed as brain dead while pregnant, speculating optimistically about what might be possible, and observing for example that “there is no known upper physiological limit to the prolongation of somatic function in the absence of brainstem function”. But this simply means we have virtually no evidence, because it’s never been done. Yet Smajdor uses it to imply we could carry on keeping the body going indefinitely. She seems to grasp at any shred of evidence that WBGD can be done. Yet at the same time, any arguments against it are dismissed as mere “distaste”.
The body is seen as a robotic resource, as a machine. The use of reason in this paper shows an instrumental rationality which understands the human body as simply part of the material universe, one more resource to be exploited and used, and as in need of improvement. The fact that even normal pregnancies are not risk free is used as an argument to justify using WBGD for any pregnancy, not simply in cases where an individual or couple cannot otherwise carry and birth a baby. But this is one place where Smajdor’s “rationality”, her mathematical calculation approach to ethics, comes apart – mysteriously, she never explains how eggs are extracted from a woman’s body, because that would remind us of the not inconsiderable risks of egg donation. Oddly as I have often noticed in much bioethics and discussions of technology ethics, it so often seems to be risks that occur in the natural course of life which are counted; risks caused by technology itself are either ignored, or it is assumed that improvements in technology can eliminate them.
Pregnancy, no; injecting a woman with massive amounts of hormones and other drugs to induce ovulation and egg extraction, yes.
The last comment for now concerns the child. Smajdor’s arguments address the physical health and safety of the foetus as it may develop within the womb of a woman who is brain-dead. Naturally physical health is extremely important. But again, she reduces the human being to nothing more than a biological, material creature. If a woman has become simply a “bio” version of a gestation machine, if she is brain dead, the baby born in such circumstances emerges from a static, unconscious and unfeeling mother. What emotional and psychological issues might this bring?
Children now often see their own ultrasounds from when they were in the womb. Recent celebrity same-sex male couples have shown off such ultrasounds, strangely isolated images, the mother entirely absent. The woman who bore a child in its first months from conception to birth is notable by her absence. What lack might such children grow to feel when they finally understand their origins? And what lack might a child feel who is born of a brain-dead donor, kept alive on ventilation for the entire period of gestation?
In surrogacy from WBGD, this is not parallel with those thankfully rare cases where a pregnant woman suffers some calamity and the pregnancy is sustained after a diagnosis of brain death to produce a child that she had wanted as her own. For in cases of WBGD surrogacy, under this scheme of technical rationality, a scheme which treats bodies as bits and pieces, and as machines to be exploited, the brain-dead woman is used as if she simply as an incubator or useful storage unit.
Of course she is never that. There are intimate biological links between a woman and the child she carries, even in the absence of any genetic relatedness. Fine-tuned adjustments to the mother’s physiology occur. Communication between mother and child takes place on many different levels. Free foetal DNA enters the maternal bloodstream. Stem cells from the foetus can help repair the mother. The growing child will recognise sounds, the mother’s voice, different tastes, the pace of the mother’s gait.
The consent of the woman to WBGD does nothing to remove these facts of human development or their significance. To focus on consent as a means of resolving ethical problems is again to see the question in terms of an abstract rationality, not in terms of the grounded biological reality and connectedness to each other which forms the underpinning of our mortal existence, which frames our moral compass.
In some jurisdictions, the families of those who donate organs may be sent anonymous “thank you” cards, or be updated anonymously about the welfare of those who received their relative’s organs. This is often a source of comfort, but must be handled with sympathy and sensitivity as families may feel their loved one “lives on” in others. With whole body gestational donation, these relatives will have waited months and months to bury their relative. What of their feelings about the child?
At birth, the child will be removed from the womb, and, presumably, the ventilation will be switched off. Will Smajdor and her bioethical colleagues tell us that concern for this is based on “irrational” feelings about the “liminal” states at the start of life, on “disgust” which we must overcome?
Arguments are sometimes presented as more rational, the more they abstract from reality they become; the more “emotional” the response the more it is dismissed or belittled. Good luck bringing up a baby on such a regime of pure reason.
Will it be left to the rest of us to explain that, no, human beings are not simply biological creatures to be manufactured to order; the dead are not simply vessels to be used to satisfy the desires of others for children. We need to explain to these “bioethicists” that, as significant as a child’s birth day is, so is their journey from inside the womb of great significance, and not just to the child but to the mother; just as the journey we all take out of this life is significant, and not just to the individual, but to all who love and care for us.
~ Paula Boddington is a moral philosopher. Paula has published on a wide variety of topics including the ethics of organ donation and transplantation, clinical genetics and genomics, and the ethics of new technologies.
Ten years ago I was a gestational surrogate for a family member on the understanding that I would have ongoing contact with the child that I would give birth to. Naively, I did not realise that this would not be a guaranteed in our arrangement. Had I known that it would not be guaranteed I would never have agreed to be a surrogate. I believe I was lied to, manipulated and exploited because somebody needed my uterus.
Surrogacy – being pregnant and having drugs injected into you daily for three months – is not an easy or pleasant experience at all. It inflicts enormous physical demands onto the body and the psychological damage is irreparable. My experience is testament to that. From the moment I was pregnant I was made to feel as though my body was no longer mine and I had no control over it. I was told what to eat and the freedoms around some of my daily routines were completely destroyed. But the worse was yet to come.
As soon as the child was born, I was abandoned by the very people I had helped and was made to feel utterly irrelevant to the child I had given birth to. This whole process had a devastating impact on my mental health to the point I was admitted into psychiatric care.
Anybody would have thought it would have been at this point that support and help would have been given to me, but no, instead the laws allowed for my mental health to be used against me, I was silenced and my consent disregarded so that parental order could be granted.
Unfortunately for those that tried to undermine me, a psychiatrist was employed to ascertain as to whether I had the capability to consent. My ability to consent was established but by this time, after all the abuse I had sustained, it was now difficult for me to give my free and unconditional consent.
I asked for a contact order but was told I would not be granted one as this would have deemed this as a condition. But the condition was central to the original understanding. It didn’t matter. I was then threatened with paying Child Maintenance by CAFCASS if I did not consent to the parental order. (I do not believe CAFCASS should ever be involved in surrogacy cases.) After being threatened, bullied and given endless false promises I relented, as my mental and physical health could take no more. I gave my consent and my parental rights were transferred to her and her husband. To this day I have never seen the child I gave birth to.
This continues to have a devastating impact on my life, I am not sure how I can live without giving birth to a child I will never see. It is not a situation I had ever envisaged I would be in as I would never had agreed to be her surrogate if this was the arrangement. I do not agree with surrogacy, I believe it should be banned completely as there is no pathway for it to ever be safe. It destroys lives and the cost not only to myself, but to many others, has been too great.
The amount of money spent on this by the tax payer should not be ignored either. I have not been able to work, I have been under the care of the NHS for ten years. All of that expense has never been directed to the commissioning parents. It has come from you, the very people who are reading this. That is completely unacceptable.
The Law Commission recent recommendations make no reassurances that what happened to me could not happen to someone else. Instead, they make it more likely. Surrogacy needs to be banned around the world, before more people are exploited and it needs to happen now.
Pro surrogacy lobbyists will say that surrogacy isn’t a job but when it is compared to forms of labour it is always to the riskier jobs. Comparisons are made to say, being a firefighter or police officer, but comparisons are never made to other service providers such as being a dentist or a cleaner. We know those roles are low-risk, so it’s subtle but we recognise there is an inherent risk in engaging in pregnancy for others.
With risky employment comes training, health and safety equipment and sometimes a significant risk allowance. If surrogacy was to be thought of as a job then there would be some health and safety guidelines, checks and an uptick in salary. And being pregnant is 24/7 with no breaks and jobs with long hours, like truck divers, rest breaks are scheduled for health and safety. Also, the riskiest jobs in the world have an element of knowingly putting yourself in harm’s way and this becomes part of the deal, and perhaps part of the draw.
With limited research in this area we rely mostly on anecdotal evidence and we have observed some common trends. Surrogate mothers will often have former careers in childcare, teaching, midwifery or nursing, and it seems to be fairly common for surrogate mothers to go on to become deeply involved in surrogacy ‘community’ and subsequently switch careers.
A small 2022 study * from a pro-surrogacy Academic, Dr Kirsty Horsey confirms that most surrogacy ‘teams’ meet through an agency as strangers and though only 47 surrogate mothers completed the survey their careers included midwifery, teaching and nursing:
“Regarding occupation, 12 surrogates identified as being in nursing, midwifery, or health care, seven were in teaching or childcare professions, and 11 in business administration, management, or accounts. Three were solicitors. Other roles included civil servant, police staff, a registrar, a hotelier, a retail role, two students, and two ‘stay-at-home moms’.”
The survey summarises that “Most responses (85%) indicated household incomes below £70,000. Four surrogates said their household incomes were above £80,000.” But it’s worth pointing out that 44 respondents answered that question and a quarter (25%) said they were on a joint income of less than £29k and another 30% said there were on a joint income of between £29k-40k. So that’s over half (55%) who are on significantly less than 70k. The footnotes for this suggests is was badly worded.
And there is a disclaimer: “Given the different professions identified, it is unclear if all respondents gave an answer reflecting personal or household incomes, suggesting that both should have been asked for in the survey. Because of this, it is unclear what weight can be given to these answers.” (Footnote 31.)
These trends bear out in real life further, these example shows that surrogate-mother-to-agency-employee pipeline is real. Take Gina Kinson for example. Having worked in nursing, Gina, a two-time surrogate mother, later became a Co-ordinator for My Surrogacy Journey. Or Sarah Jones, now CEO of Surrogacy UK, Sarah is an Early Years Educator and has had 5 babies for others. Another is Dawn Allen, a surrogate applications and agreement Co-ordinator for Surrogacy UK. Initially inspired to have babies for others after watching a documentary, Dawn came out of ‘retirement’ to have a baby for a couple at the age of 49 whilst working at Surrogacy UK.
So it appears common that a surrogate mother’s career will centre, at least for some, around care-giving and providing a service and having had a baby for others can result in becoming more deeply involved in the industry.
If surrogacy is a vocation where you provide a service in exchange for money, it’s a regular job like any other and one you can retire from. It’s not just ‘favour’ you do for a friend or family member, not least because women are having babies for strangers they are matched with. Surrogacy is no longer what we thought it was when it began back in the 80s. (You may have seen #changingthelandscape used on pro-surrogacy posts and they are not wrong, the landscape has indeed changed.)
In risky jobs we assess and name the risks using clear language in the job description so applicants know what the role entails. (Prostitution isn’t a job, but we have seen it be more commonly referred to as ‘sex work’, as a way to normalise and rationalise the act of using a woman’s body for paid rape as job she chooses to do or a ‘vocation’.) Now there are subtle shifts in language in surrogacy too. Agencies now refer to ‘compensation’ rather than the legal term of ‘reasonable expenses’.
Pregnancy and labour is unpredictable and carries risk. We don’t currently consider surrogacy as a form of employment in the UK, as ‘contracts’ are not enforceable (though that’s a whole different blog), but monetising women’s bodies is a slippery slope.
If you have concerns about surrogacy becoming more widespread, the impact on women and children and what proposed reform in the UK would lead us, please get in contact.
** With 47 respondents to this 2022 survey, this could be roughly just 10% of parental orders as 449 Parental Orders were granted in 2022.
There has been an interesting response to the Royal College of Midwives (RCM) webinar on Surrogacy. Perhaps it’s not surprising that those ‘with women’ wanted to offload their or share what they themselves have witnessed when supporting patients through pregnancy, birth ‘and beyond’.
Midwives got in touch with us to tell us of their shock at when they heard their union was considering hosting a webinar on surrogacy. We later heard from the women who attended that it was far from a the ‘neutral’ presentation they were promised.
Parts One and Two of this short blog series are direct accounts from RCM Members who attended and who remain anonymous and other midwives gave us permission to share their personal perceptions of surrogacy in their day-to-day jobs.
A Community Midwife noticed how the glossy images a surrogate mother posted online which promoted surrogacy as a wholly positive experience hid the very raw and real realities of her birth injuries.
Another midwife said something similar about a woman who had a baby for a family member. The commissioning mother was posting on social media about how amazing her ‘journey’ was, but this midwife knew the reality for the birth mother. It was filled with gestational diabetes (which can lead to higher risk of diabetes in future), obstetric cholestasis which is a liver condition (that can causes liver disease and other issues in the future) and high blood pressure. This risky pregnancy ended in a C section. The truth was this woman was devastated after the birth as she would never have another child of her own due to these complications. It put a strain on her own marriage as her husband, while initially supportive, didn’t realise the enormous negative affect this had on his wife’s health and the future of their own family. This desperately sad reality was not shared on social media.
Another midwife commented on the late maternal age of two surrogate mothers she cared for and she expressed concern that there are no upper age limits in proposed reform. Both of the surrogate mothers she supported were in their 50s. She felt that as the pool of women available for surrogacy was ‘slim pickings’, women with a complex obstetric histories may be considered by the commissioning parents as their options were limited. This was nothing to say of the risk to the baby.
And finally there was one patient that stayed in the mind of a midwife we spoke to by phone. She told us how she supported this woman through four surrogacy pregnancies. The midwife knew she had lost touch with all but one of the families she was pregnant and gave birth for. During these pregnancies the commissioning parents were her “best friends” but once the baby had been delivered, the surrogate mother was “ghosted” and she then grieved the loss of the lifelong friendship she was told she could rely on.
In sharing their experiences these midwives has a sense of release, as if they had to keep to the official line outwardly, but inwardly there was worry and anger building as they were unable to talk freely. In our conversations these women were able to air their concerns about the direction of travel of surrogacy in the UK. Several felt badly let down by their union as women and as midwives.
We were left with a distinct observation that midwives are on the ‘front line’ of surrogacy. Any legal disputes may end up in the court room but they begin on a maternity ward. It is the midwives and other healthcare professionals who will have to navigate the practicalities on the ground around consent, the removal of the newborn and ongoing mental and physical health problems as a result of surrogacy births.
Following the Royal College of Midwives webinar on Surrogacy last week, a Midwife got in touch with us to share her experience and her concerns about what the promotion of surrogacy in midwifery means for her. To protect her identity we share the following without sharing her name.
As an RCM member for the past 28 years, I’ve always felt my union has had my best interests at heart. I’ve felt confident of their support and on the very few occasions I’ve needed their assistance, they haven’t let me down. But now I feel things may be starting to change, and I’m deeply concerned.
I attended their webinar last week which was advertised online as a discussion on surrogacy and how we, as midwives can support parents of babies born of surrogate mothers. The subject of surrogacy troubles me but the content shocked me.
Since I was a teenager at the start of my training, it is embedded into the heart of what it is to be a Midwife and that is to be ‘with mother’. Our role is to be her closest carer and her biggest advocate – yet here we were being told in this new way, she is not a mother, but a ‘carrier of a baby’. A baby who is to be given away at birth, and not only that, our care as midwives should be transferred over to these ‘intended parents’.
It was very clear as soon as the webinar started that this was not a discussion or a debate on surrogacy, but well thought-out propaganda on the wonders of surrogacy, with stories from a surrogate mother and two parents of children born through surrogacy.
There are no official stats on how many children are born through surrogacy in the UK. There is no disclosure on prospective parents and we know just by reading the news, that people from the UK are traveling abroad to buy babies. Although women in the UK are not paid for their ‘reproductive service’ there are incentives and ‘independant journeys’ (private arrangements) are being made online. If you’re lucky you get an Apple Watch and Ann Summers vouchers among other goodies from an agency. When someone in the chat questioned the ethics of this, they were told by the owners (two men) that it’s nice for the surrogate to have the Ann Summers vouchers to spice things up with her partner as she can’t have penetrative sex when pregnant. Oh how we laughed, does anyone want to tell them? Questions that criticised this controversial practice largely went unanswered.
The surrogate mother and CEO of another agency, Surrogacy UK, told her story of carrying 5 babies for other people, some her own eggs, some not and once during COVID. She was asked if she was concerned for her own health and well-being due to the risks of the amount of IVF pregnancies she’d put her body through. She said she made fully informed decisions by speaking to her obstetrician and was aware of the risks and happy to take them. It’s worth noting that the long term implications cannot be known but that multiple cycles of IVF have been shown to increase the risk of ovarian and uterine cancers. Not to mention the risk of vaginal/rectal/cervical prolapse in later years following so many pregnancies. Along with her other children this woman had a total of 8 pregnancies and births including 2 c sections.
The two men who were advocates for surrogacy having had two children by arranged births and egg donation and they have their own agency and have recently expanded into Mexico City. Promoting surrogacy and offering the incentives discussed, they talked about the horrendous experience they had of the surrogate being called the mother by a Midwife and that their name could not appear on the ID band of the baby in hospital. It’s worth noting that unless a couple have the same surname, the baby will always have the mother’s name on the ID band. This is not to offend or irritate but for the basic security and safeguarding of the baby in case of a mix up or kidnapping. They were quite proud to announce that the health board crumbled at their request and they got to put their names on the ID band. Who cares about safeguarding for babies anyway eh?
My biggest concern is the long term implications for the birth mother and the baby. A baby who has known nothing but their mother’s heartbeat, her voice, her body for 40 weeks, only to be taken away and placed with strangers. And for the mother, who needs her child close to her for both their wellbeing, to regulate temperature and heart rate, to stimulate feeding instincts, to contract the womb, minimise bleeding and to release oxytocin to reduce the risk of postnatal depression and complications.
I know there are instances where this is unavoidable, but we shouldn’t as midwives, be promoting this as the norm. I don’t provide postnatal care to adoptive parents or to foster parents, so why am I being asked to treat these ‘intended parents’ as if they are the ones who have given birth? That is not my role as a midwife.These people are not my patients.
I am heartened by the fact that the student midwives I’ve spoken to feel that surrogacy is a problem in modern society. This seems to be due to the boom in celebrity surrogacy where it is clear the rich and famous are exploiting poor and vulnerable women, using them as a ‘vessel’ to carry a baby to avoid putting their own bodies through the trauma of childbirth. And the grotesque fad of lying on a hospital bed, as through they have just given birth themselves, is doing nothing to convince our new recruits that this transaction is anything other than a horrendous experience for the mother who has just given birth, and for the baby who has been removed from his or her mother literally seconds after being born. Sickeningly, there are numerous photos of babies still attached to the umbilical cord with the placenta still inside the womb, as the smiling commissioning parents hold this newly delivered baby that is crying out for their mother.
I have been taught a research-based approach throughout my career and to apply critical thinking whenever there is discussion or debate. Yet there was no other side to this webinar and the questions examining the other side were ignored. No known long term implications to the child born of surrogacy were discussed, no evidence of a long term follow up for women who have given their bodies and their babies to others. And no matter if surrogacy is commercial or altruistic, arranged on facebook or through an agency, if the mother uses her own egg or if the embryo has been conceived with a donor’s eggs, the social and moral outcome is the same.
A baby has been taken from his or her mother at birth.